
Introduction
Hair loss, or alopecia, affects millions globally and is a significant health concern. Among the various forms of hair loss, androgenetic alopecia, commonly known as male or female pattern baldness, is the most prevalent. It is characterized by gradual thinning and progressive hair follicle miniaturization, driven predominantly by genetic factors and hormonal influences (1; 2; 3).
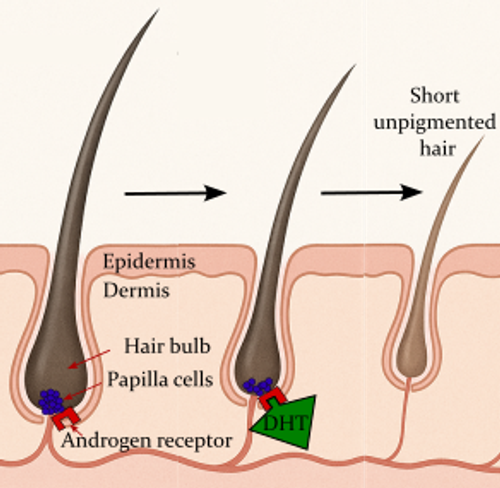
Figure 1: How DHT affects hair growth
This illustration shows how the hormone dihydrotestosterone (DHT) can contribute to hair thinning and loss. In healthy hair follicles (left), the hair grows thick and dark. Over time, DHT binds to androgen receptors in the hair bulb’s papilla cells (purple), which are located at the base of the follicle. This interaction causes the hair follicle to shrink, producing shorter, thinner, and lighter (unpigmented) hair, as seen on the right side of the image. Eventually, the follicle may stop producing visible hair altogether.
Hair loss is not a uniquely modern concern; rather, it has persisted across diverse cultures throughout history. In medieval Europe, extensive attention was given to hair health, with medical texts from the 12th to 14th centuries proposing detailed theoretical explanations and practical remedies based on humoral theory to manage baldness and greying (7). Similarly, traditional Chinese medicine, dating back to the Qin and Han dynasties, initially attributed hair loss to bodily deficiencies and external pathogenic influences, evolving over centuries to more sophisticated theories involving liver and kidney insufficiency, qi and blood deficiency, and blood stagnation (8). Remedies in both traditions predominantly utilized herbal and natural compounds, underscoring a longstanding reliance on holistic and regionally tailored treatments designed to restore bodily balance (9; 10).
Pharmaceutical intervention
Pharmaceutical intervention is effective in treatment for androgenetic alopecia, with the most robust evidence supporting two FDA-approved agents: finasteride and minoxidil (see figure 2). Finasteride, a type II 5α-reductase inhibitor, reduces the conversion of testosterone to DHT, thereby mitigating hair follicle miniaturization and promoting anagen phase extension (11; 12; 13; 14). Clinical trials have consistently demonstrated that oral finasteride (1 mg/day) significantly increases hair count, reduces hair loss, and improves hair appearance in men, with effects maintained over long-term use (15; 11; 16). However, oral finasteride is associated with a range of potential side effects, including sexual dysfunction (decreased libido, erectile dysfunction), mood changes, and rarely, depression and persistent post-finasteride syndrome in some users (11; 12; 14). Topical finasteride formulations aim to reduce systemic absorption and minimize these adverse effects while maintaining efficacy (17; 18).
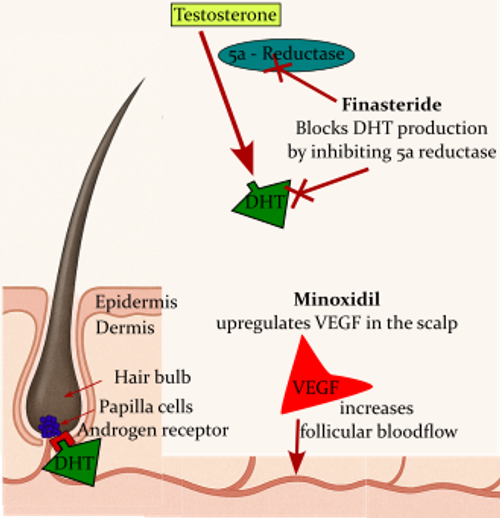
Figure 2: Mechanisms of action of finasteride and minoxidil in hair loss treatment
This diagram illustrates how finasteride and minoxidil help combat hair loss. In the hair follicle, testosterone is converted into dihydrotestosterone (DHT) by the enzyme 5α-reductase. DHT binds to androgen receptors in papilla cells at the base of the follicle, leading to follicle shrinkage and hair thinning. Finasteride works by inhibiting 5α-reductase, reducing DHT production and thereby preventing further follicle damage. Minoxidil acts through a different mechanism: it increases the production of vascular endothelial growth factor (VEGF) in the scalp, which enhances blood flow to the follicle, supporting healthier hair growth.
Combination therapies, such as finasteride plus minoxidil or minoxidil with platelet-rich plasma (PRP), have shown additive or synergistic benefits, enhancing hair regrowth and retention compared to monotherapy (22; 23). Advances in delivery systems, including nanotechnology and phospholipid vesicles, aim to enhance follicular targeting and minimize systemic absorption (22). Emerging pharmaceutical interventions, such as topical prostaglandin analogues (e.g., latanoprost and bimatoprost), Janus kinase (JAK) inhibitors (e.g., tofacitinib), and oral dutasteride (a dual 5α-reductase inhibitor), are under investigation for androgenetic alopecia and other forms of hair loss (14; 24; 25). While these agents show promise by targeting various molecular pathways, their safety profiles, particularly for systemic agents like JAK inhibitors, require cautious evaluation due to potential risks including immunosuppression and increased infection risk (24).
Lifestyle factors in hair loss and growth
Lifestyle factors play a pivotal role in both the progression and potential mitigation of hair loss, including androgenetic alopecia. Smoking has been identified as a modifiable risk factor, with evidence showing that smokers have higher odds of experiencing hair loss, particularly androgenetic alopecia (26). Mechanistically, smoking induces vascular constriction, reduces blood flow to hair follicles, and increases oxidative stress and inflammatory cytokines, all of which can accelerate follicular miniaturization and hair loss (27; 28). Additionally, smoking alters hormone metabolism and contributes to follicular DNA damage (29; 30), compounding the risk.
Dietary factors also modulate hair health. Nutrient-rich diets, particularly those aligned with the Mediterranean pattern (rich in vegetables, fresh herbs, and anti-inflammatory nutrients) have been linked to lower risks of androgenetic alopecia (31). Adequate intake of proteins, vitamins (e.g., A, B complex, C, D, E), minerals (e.g., zinc, iron, selenium), and antioxidants supports the hair growth cycle and counteracts oxidative stress, whereas deficiencies can exacerbate hair thinning and loss (32; 33). Furthermore, animal studies suggest obesity and high-fat diets negatively influence hair follicle stem cell function and promote inflammation, contributing to hair loss progression (34).
Psychological stress is another critical lifestyle factor. Chronic stress elevates cortisol and pro-inflammatory neuropeptides, which disrupt hair follicle cycling by promoting premature regression (catagen) and inhibiting regrowth (anagen) (35; 36). High stress levels have been linked to poorer responses to treatments like minoxidil and to faster progression of hair thinning (37). Emerging research suggests potential benefits of stress-reduction interventions, including stress management and even topical pharmacologic agents such as propranolol (38).
Finally, several aspects of routine hair care have been shown to affect hair loss/regrowth. Mechanical scalp stimulation, including manual scalp massage and device-assisted techniques, has shown promise in improving hair thickness and scalp health. While evidence is mostly limited to small studies and self-reported outcomes, standardized scalp massage has been associated with increased hair shaft diameter and stabilization of hair loss in individuals with androgenetic alopecia (39; 40). Additionally, essential oils such as rosemary, peppermint, lavender, and Ocimum gratissimum are increasingly used to promote hair growth, with mechanisms including antioxidant effects, improved scalp circulation, and hormonal modulation (41; 42). Rosemary oil has shown some human trial efficacy, while others like peppermint have promising animal data, but overall evidence remains limited (43; 44). Products containing these oils may improve hair density and strength, though risks like irritation exist and more robust clinical trials are needed (45). Finally, topical caffeine is emerging as a potentially useful ingredient in shampoos and hair care products, with trials reporting increases in hair density and reduction in hair shedding (46).
Nutraceuticals/supplements
Nutraceuticals, defined as dietary supplements offering potential health benefits, have been widely explored for their role in supporting hair health and addressing androgenetic alopecia. Deficiencies in key micronutrients, including vitamin D, iron, zinc, and B vitamins, have been associated with various forms of hair loss such as androgenetic alopecia, telogen effluvium, and alopecia areata (47; 48). Correcting such deficiencies has been shown to improve hair regrowth outcomes, but evidence for supplementation in non-deficient individuals remains inconsistent and inconclusive (47; 48; 49; 50).
Saw palmetto, derived from Serenoa repens, has garnered attention as a natural alternative to finasteride due to its 5-alpha-reductase inhibition properties. Clinical studies, though limited in size and design, suggest saw palmetto may modestly improve hair growth and quality, particularly in vertex regions of the scalp (55; 56; 57). However, its efficacy appears inferior to standard pharmacotherapies, and larger trials are needed to establish definitive benefit. Marine protein supplements, such as Viviscal, contain ingredients like shark cartilage and mollusk powder, aiming to stimulate dermal papilla cells and enhance hair growth. Industry-funded randomized controlled trials have reported improvements in hair count and quality, especially in women with thinning hair (58; 59), though effects are generally modest and sample sizes limited.
Pumpkin seed oil (PSO) offers another natural option, leveraging its phytosterol content to inhibit 5-alpha-reductase and reduce DHT levels. Small human and animal studies report increased hair counts and reduced hair loss with PSO supplementation, though the scale and duration of these trials limit generalizability (60; 61). Collagen peptides are increasingly used to promote hair thickness and strength by enhancing dermal papilla cell proliferation and stimulating growth factors such as IGF-1 and VEGF (62; 63). Clinical studies report improved hair structure and mechanical properties, though further validation is needed. Similarly, combinations like capsaicin with isoflavones have demonstrated enhanced hair regrowth in early studies, potentially via increased local IGF-I production (64; 65).
Finally, zinc, an essential trace element, is vital for hair follicle health. While deficiency is linked to hair loss, supplementation without confirmed deficiency may offer limited benefits (67; 68). Emerging delivery methods, such as zinc-containing microneedle patches, show promise in enhancing zinc bioavailability and promoting hair regrowth (68).
Overall, while nutraceuticals present intriguing options for managing androgenetic alopecia, their effects are generally modest, and robust evidence from large-scale, controlled studies is still lacking. Many of these supplements lack sufficient participant numbers or have competing interests from industry funding. Nevertheless, most of these supplements have a good safety profile compared to pharmaceutical intervention. See Table 1 for a summary of the available evidence.
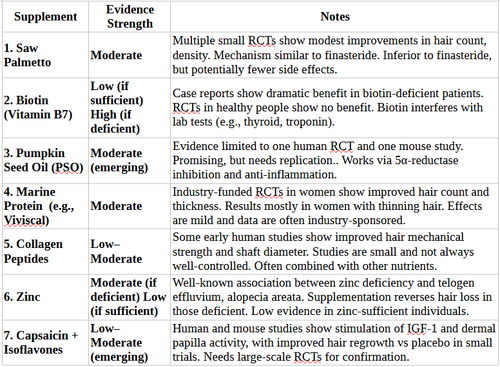
Table 1. Summary of the available evidence for the role of various supplements in hair re-growth
Conclusion: Navigating the Hair Growth Landscape with Science and Strategy
Hair loss, especially androgenetic alopecia, is a complex puzzle with no one-size-fits-all solution. While pharmaceutical interventions like finasteride and minoxidil offer proven results for many, they come with caveats: potential side effects, the need for lifelong use, and variable efficacy. For those seeking alternatives or complementary strategies, lifestyle changes, targeted nutraceuticals, and mindful self-care offer a holistic approach. Emerging data supports that factors like smoking, poor nutrition, chronic stress, and scalp tension accelerate hair loss, while a nutrient-rich diet, stress management, and even mechanical scalp stimulation can create a more favorable environment for hair regrowth. Natural options like saw palmetto, pumpkin seed oil, and essential oils also show promise, though unbiased evidence is still catching up with the hype.
References
- Fu, D., Huang, J., Li, K., Chen, Y., He, Y., Sun, Y., Guo, Y., Du, L., Qu, Q., Miao, Y., & Hu, Z. (2021). Dihydrotestosterone-induced hair regrowth inhibition by activating androgen receptor in C57BL6 mice simulates androgenetic alopecia.. Biomedicine & pharmacotherapy = Biomedecine & pharmacotherapie, 137, 111247.
- Premanand, A., & Rajkumar, R. (2018). Androgen modulation of Wnt/β-catenin signaling in androgenetic alopecia. Archives of Dermatological Research, 310, 391-399.
- Owecka, B., Tomaszewska, A., Dobrzeniecki, K., & Owecki, M. (2024). The Hormonal Background of Hair Loss in Non-Scarring Alopecias. Biomedicines, 12.
- Alsantali, A., & Shapiro, J. (2009). Androgens and hair loss. Current Opinion in Endocrinology, Diabetes and Obesity, 16, 246–253.
- Devjani, S., Ezemma, O., Kelley, K., Stratton, E., & Senna, M. (2023). Androgenetic Alopecia: Therapy Update. Drugs, 83, 701 - 715.
- English, R. (2018). A hypothetical pathogenesis model for androgenic alopecia: clarifying the dihydrotestosterone paradox and rate-limiting recovery factors.. Medical hypotheses, 111, 73-81.
- Lisowska, K. (2023). Hair Care in the Light of Selected Medieval Medical Treatises. Respectus Philologicus.
- Ji, Z. (2014). Historical Evolution on Hair Loss in Treatment with Traditional Chinese Medicine. World Journal of Integrated Traditional and Western Medicine.
- Gasmi, A., Mujawdiya, P., Beley, N. et al. (2023). Natural Compounds Used for Treating Hair Loss. Current Pharmaceutical Design.
- Świątkul, A., Polakowska, N., Głavač, K. & Kreft, S. (2019). Herbal preparations for the treatment of hair loss. Archives of Dermatological Research, 312, 395-406.
- Kaufman, K., Olsen, E., Whiting, D., Savin, R., Devillez, R., Bergfeld, W., Price, V., Nester, D., Roberts, J., Hordinsky, M., Shapiro, J., Binkowitz, B., & Gormley, G. (1998). Finasteride in the treatment of men with androgenetic alopecia. Finasteride Male Pattern Hair Loss Study Group.. Journal of the American Academy of Dermatology, 39 4 Pt 1, 578-89.
- Leyden, J., Dunlap, F., Miller, B., Winters, P., Lebwohl, M., Hecker, D., Kraus, S., Baldwin, H., Shalita, A., Draelos, Z., Markou, M., Thiboutot, D., Rapaport, M., Kang, S., Kelly, T., Pariser, D., Webster, G., Hordinsky, M., Rietschel, R., Katz, H., Terranella, L., Best, S., Round, E., & Waldstreicher, J. (1999). Finasteride in the treatment of men with frontal male pattern hair loss.. Journal of the American Academy of Dermatology, 40 6 Pt 1, 930-7.
- Neste, D., Fuh, V., Sänchez-Pedreño, P., Lópe64z-Bran, E., Wolff, H., Whiting, D., Roberts, J., Kopera, D., Stene, J., Calvieri, S., Tosti, A., Prens, E., Guarrera, M., Kanojia, P., He, W., & Kaufman, K. (2000). Finasteride increases anagen hair in men with androgenetic alopecia. British Journal of Dermatology, 143.
- Gupta, A., Talukder, M., & Williams, G. (2022). Comparison of oral minoxidil, finasteride, and dutasteride for treating androgenetic alopecia. Journal of Dermatological Treatment, 33, 2946 - 2962.
- Adil, A., & Godwin, M. (2017). The effectiveness of treatments for androgenetic alopecia: A systematic review and meta-analysis. Journal of the American Academy of Dermatology, 77, 132–141.e5.
- Whiting, D., Waldstreicher, J., Sanchez, M., & Kaufman, K. (1999). Measuring reversal of hair miniaturization in androgenetic alopecia by follicular counts in horizontal sections of serial scalp biopsies: results of finasteride 1 mg treatment of men and postmenopausal women.. The journal of investigative dermatology. Symposium proceedings, 4 3, 282-4.
- Piraccini, B., Blume-Peytavi, U., Scarci, F., Jansat, J., Falqués, M., Otero, R., Tamarit, M., Galván, J., Tebbs, V., & Massana, E. (2021). Efficacy and safety of topical finasteride spray solution for male androgenetic alopecia: a phase III, randomized, controlled clinical trial. Journal of the European Academy of Dermatology and Venereology, 36, 286 - 294.
- Nobari, N., RoohaniNasab, M., Sadeghzadeh-Bazargan, A., Goodarzi, A., Behrangi, E., Nikkhah, F., & Ghassemi, M. (2023). A systematic review of clinical trials using single or combination therapy of oral or topical finasteride for women in reproductive age and postmenopausal women with hormonal and nonhormonal androgenetic alopecia.. Advances in clinical and experimental medicine : official organ Wroclaw Medical University.
- Messenger, A., & Rundgren, J. (2004). Minoxidil: mechanisms of action on hair growth. British Journal of Dermatology, 150.
- Suchonwanit, P., Thammarucha, S., & Leerunyakul, K. (2019). Minoxidil and its use in hair disorders: a review. Drug Design, Development and Therapy, 13, 2777 - 2786.
- Vázquez-Galván S, Primez R, Hermosa-Gelbard A, Moreno-Arrones ÓM, Saceda-Corralo D, Rodríguez-Barata R, Jimenez-Cauhe J, Koh WL, Poa JE, Jerjen R, Trindade de Carvalho L, John JM, Salas-Callo CI, Vincenzi C, Yin L, Lo-Sicco K, Waskiel-Burnat A, Starace M, Zamorano JL, Jean-Olasolo P, Piraccini BM, Rudnicka L, Shapiro J, Tosti A, Sinclair R, Bhoyrul B. Safety of low-dose oral minoxidil for hair loss: A multicenter study of 1404 patients. J Am Acad Dermatol. 2021 Jun;84(6):1644-1651. doi: 10.1016/j.jaad.2021.02.054. Epub 2021 Feb 24. PMID: 33639244.
- Mir-Palomo, S., Nàcher, A., Vila-Busó, M., Cañedo, C., Manca, M., Sauri, A., Escribano-Ferrer, E., Manconi, M., & Dérrez-Sales, O. (2020). Co-loading of finasteride and baicalin in phospholipid vesicles tailored for the treatment of hair disorders.. Nanoscale.
- Diani, A., Mulholland, M., Shull, K., Kubicek, M., Johnson, G., Schostarez, H., Brunden, M., & Buhl, A. (1992). Hair growth effects of oral administration of finasteride, a steroid 5 alpha-reductase inhibitor, alone and in combination with topical minoxidil in the balding stump-tail macaque.. The Journal of clinical endocrinology and metabolism, 74 2, 345-50.
- Gilhar, A., Keren, A., & Paus, R. (2019). JAK inhibitors and alopecia areata. The Lancet, 393, 318-319.
- Lensing, M., & Jabbari, A. (2022). An overview of JAK/STAT pathways and JAK inhibition in alopecia areata. Frontiers in Immunology, 13.
- Gupta, A., Bamimore, M., & Talukder, M. (2024). A meta‐analysis study on the association between smoking and male pattern hair loss. Journal of Cosmetic Dermatology, 23, 1446 - 1451.
- Trüeb, R. (2003). Association between Smoking and Hair Loss: Another Opportunity for Health Education against Smoking?. Dermatology, 206, 189 - 191.
- Kavadyia, Y., & Mysore, V. (2022). Role of Smoking in Androgenetic Alopecia: A Systematic Review. International Journal of Trichology, 14, 41 - 48.
- Ahmed, A., Aldubayan, M., Ahmed, H., Refaat, A., Alsalloum, A., Almasuood, R., & Elgharabawy, R. (2020). Impact of smoking on heavy metal contamination and DNA fragmentation. Environmental Science and Pollution Research, 28, 13931 - 13941.
- D'Agostini, F., Balansky, R., Pesce, C., Fiallo, P., Lubet, R., Kelloff, G., & Flora, S. (2000). Induction of alopecia in mice exposed to cigarette smoke.. Toxicology letters, 114 1-3, 117-23.
- Fortes C, Mastroeni S, Mannooranparampil T, Abeni D, Panebianco A. Mediterranean diet: fresh herbs and fresh vegetables decrease the risk of Androgenetic Alopecia in males. Arch Dermatol Res. 2018 Jan;310(1):71-76. doi: 10.1007/s00403-017-1799-z. Epub 2017 Nov 27. PMID: 29181579.
- Pham, C., Romero, K., Almohanna, H., Griggs, J., Ahmed, A., & Tosti, A. (2020). The Role of Diet as an Adjuvant Treatment in Scarring and Nonscarring Alopecia. Skin Appendage Disorders, 6, 88 - 96.
- Rajput, R. (2022). Influence of Nutrition, Food Supplements and Lifestyle in Hair Disorders. Indian Dermatology Online Journal, 13, 721 - 724.
- Moringa, H., Mohri, Y., Grachtchouk, M., Asakawa, K., Matsumura, H., Oshima, M., Takayama, N., Kato, T., Nishimori, Y., Sorimachi, Y., Takubo, K., Suganami, T., Iwama, A., Iwakura, Y., Dlugosz, A., & Nishimura, E. (2021). Obesity accelerates hair thinning by stem cell-centric converging mechanisms. Nature, 595, 266 - 271.
- Liang, W., Zhao, Y., Cai, B., Huang, Y., Chen, X., Ni, N., Wang, Y., Lin, Z., Lin, C., & Huang, K. (2024). Psychological stress induces hair regenerative disorders through corticotropin-releasing hormone-mediated autophagy inhibition.. Biochemical and biophysical research communications, 699, 149564.
- Arck, P., Handjiski, B., Peters, E., Peter, A., Hagen, E., Fischer, A., Klapp, B., & Paus, R. (2003). Stress inhibits hair growth in mice by induction of premature catagen development and deleterious perifollicular inflammatory events via neuropeptide substance P-dependent pathways.. The American journal of pathology, 162 3, 803-14.
- Published online Oct 19, 2024. doi: 10.5498/wjp.v14.i10.1437Psychological stress impact neurotrophic factor levels in patients with androgenetic alopecia and correlated with disease progressionYi Cheng, Li-Jing Lv, Yu Cui, Xiao-Mei Han, Yan Zhang, Cai-Xia Hu
- Zhu M, Zheng B, Zhang Y, Sun R, Xu X, Tian R, Li X, Wang G, Wang X, Liu Z. A single-center clinical trial evaluating topical propranolol for preventing stress-induced hair loss. FASEB J. 2024 Nov 30;38(22):e70191. doi: 10.1096/fj.202401027R. PMID: 39570058; PMC ID: PMC11580711.
- Koyama T, Kobayashi K, Hama T, Murakami K, Ogawa R. Standardized Scalp Massage Results in Increased Hair Thickness by Inducing Stretching Forces to Dermal Papilla Cells in the Subcutaneous Tissue. Eplasty. 2016 Jan 25;16:e8. PMID: 26904154; PMCID: PMC4740347.
- English, R., & Barazesh, J. (2019). Self-Assessments of Standardized Scalp Massages for Androgenic Alopecia: Survey Results. Dermatology and Therapy, 9, 167 - 178.
- Dinkins, J., Iwuala, C., Akintilo, L., Ugonabo, N., Shapiro, J., Sicco, K., & Adotama, P. (2023). Commonly used hair oils in the Black community: a narrative review in their use to treat androgenetic alopecia. International Journal of Dermatology, 62.
- Hussain, F., & Dubash, F. (2024). BC07 Hair oiling: a paradigm shift in the deep-rooted ritual from East to West. British Journal of Dermatology.
- Júnior, A., & Bastos, C. (2024). Essential Oils for Hair Health: A Critical Mini-Review of the Current Evidence and Future Directions. Brazilian Journal of Health Aromatherapy and Essential Oil.
- Fullas, F., Russell, S., & Hailemeskel, B. (2024). Hair Loss (Alopecia) Treatment using rosemary oil, peppermint oil, amla oil and saw palmetto: A students’ survey. International Journal of Scholarly Research in Biology and Pharmacy.
- Orafidiya, L., Agbani, E., Adelusola, K., Iwalewa, E., Adebamiji, O., Adediran, E., & Agbani, N. (2004). A study on the effect of the leaf essential oil of Ocimum gratissimum Linn. on cyclophosphamide-induced hair loss. International Journal of Aromatherapy, 14, 119-128.
- Szendzielorz, E., & Śpiewak, R. (2025). Caffeine as an Active Molecule in Cosmetic Products for Hair Loss: Its Mechanisms of Action in the Context of Hair Physiology and Pathology. Molecules, 30.
- Lee, J. (2023). A Study on Changes in Hair Condition of Shampoo Containing Aroma Essential Oil. Journal of the Korean Society of Cosmetology.
- Almohanna, H., Ahmed, A., Tsatalis, J., & Tosti, A. (2018). The Role of Vitamins and Minerals in Hair Loss: A Review. Dermatology and Therapy, 9, 51 - 70.
- Wang, R., Lin, J., Liu, Q., Wu, W., Wu, J., & Liu, X. (2024). Micronutrients and Androgenetic Alopecia: A Systematic Review.. Molecular nutrition & food research, e2400652.
- Drake, L., Reyes-Hadsall, S., Martinez, J., Heinrich, C., Huang, K., & Mostaghimi, A. (2022). Evaluation of the Safety and Effectiveness of Nutritional Supplements for Treating Hair Loss: A Systematic Review.. JAMA dermatology.
- Guo, E., & Katta, R. (2017). Diet and hair loss: effects of nutrient deficiency and supplement use. Dermatology Practical & Conceptual, 7, 1 - 10.
- [Patel DP, Swink SM, Castelo-Soccio L. A Review of the Use of Biotin for Hair Loss. Skin Appendage Disord. 2017 Aug;3(3):166-169. doi: 10.1159/000462981. Epub 2017 Apr 27. PMID: 28879195; PMCID: PMC5582478.]
- Yelich, A., Jenkins, H., Holt, S., & Miller, R. (2024). Biotin for Hair Loss: Teasing Out the Evidence.. The Journal of clinical and aesthetic dermatology, 17 8, 56-61.
- Trüeb, R. (2017). Comment on the Use of Biotin for Hair Loss. Skin Appendage Disorders, 4, 345 - 346.
- Benke, P., Duchowny, M., & McKnight, D. (2017). Biotin and Acetazolamide for Treatment of an Unusual Child With Autism Plus Lack of Nail and Hair Growth.. Pediatric neurology, 79, 61-64.
- Prager N, Bickett K, French N, Marcovici G. A randomized, double-blind, placebo-controlled trial to determine the effectiveness of botanically derived inhibitors of 5-alpha-reductase in the treatment of androgenetic alopecia. J Altern Complement Med. 2002 Apr;8(2):143-52. doi: 10.1089/acm.2002.8.143. Erratum in: J Altern Complement Med. 2006 Mar;12(2):199. PMID: 12006122.
- Rossi A, Mari E, Scarno M, Garelli V, Maxia C, Scali E, Iorio A, Carlesimo M. Comparative effectiveness of finasteride vs Serenoa repens in male androgenetic alopecia: a two-year study. Int J Immunopathol Pharmacol. 2012 Oct-Dec;25(4):1167-73. doi: 10.1177/039463201202500435. PMID: 23298508.
- Evron, E., Juhász, M., Babajouni, A., & Mesinkovska, N. (2020). Natural Hair Supplement: Friend or Foe? Saw Palmetto, a Systematic Review in Alopecia. Skin Appendage Disorders, 6, 329 - 337.
- Ablon G, Dayan S. A Randomized, Double-blind, Placebo-controlled, Multi-center, Extension Trial Evaluating the Efficacy of a New Oral Supplement in Women with Self-perceived Thinning Hair. J Clin Aesthet Dermatol. 2015 Dec;8(12):15-21. PMID: 26705444; PMCID: PMC4689507.
- Rizer, R., Stephens, T., Herndon, J., Sperber, B., Murphy, J., & Ablon, G. (2015). A Marine Protein-based Dietary Supplement for Subclinical Hair Thinning/Loss: Results of a Multisite, Double-blind, Placebo-controlled Clinical Trial. International Journal of Trichology, 7, 156 - 166.
- Cho YH, Lee SY, Jeong DW, Choi EJ, Kim YJ, Lee JG, Yi YH, Cha HS. Effect of pumpkin seed oil on hair growth in men with androgenetic alopecia: a randomized, double-blind, placebo-controlled trial. Evid Based Complement Alternat Med. 2014;2014:549721. doi: 10.1155/2014/549721. Epub 2014 Apr 23. PMID: 24864154; PMCID: PMC4017725.
- Hajhashemi, V., Rajabi, P., & Mardani, M. (2019). Beneficial effects of pumpkin seed oil as a topical hair growth promoting agent in a mice model. Avicenna Journal of Phytomedicine, 9, 499 - 504.
- Oral intake of Bioactive Collagen Peptides in the improvement of skin and hair: clinical studies by instrumental measurements Published 2022 P. M. Maia Campos, Márcia Oliveira de Melo, Marina Mendes Fossa Shirata
- Lee, J., Kim, Y., Lee, J., Suk, J., Jung, I., Choi, S., Yoo, K., Seok, J., & Kim, B. (2024). AP collagen peptides (APCPs) promote hair growth by activating the GSK-3β/β-catenin pathway and improve hair condition.. Experimental dermatology, 33 7, e15137.
- Harada, N., Okajima, K., Arai, M., Kurihara, H., & Nakagata, N. (2007). Administration of capsaicin and isoflavone promotes hair growth by increasing insulin-like growth factor-I production in mice and in humans with alopecia.. Growth hormone & IGF research : official journal of the Growth Hormone Research Society and the International IGF Research Society, 17 5, 408-15.
- Zhao, J., Harada, N., Kurihara, H., Nakagata, N., & Okajima, K. (2011). Dietary isoflavone increases insulin-like growth factor-I production, thereby promoting hair growth in mice.. The Journal of nutritional biochemistry, 22 3, 227-33.
- Martin-Biggers, J., & De Campos, M. (2024). A Randomized, Placebo-controlled Clinical Study Evaluating a Dietary Supplement for Hair Growth.. The Journal of clinical and aesthetic dermatology, 17 11, 34-38.
- Yang, Y., Wang, P., Gong, Y., Yu, Z., Gan, Y., Li, P., Liu, W., & Wang, X. (2023). Curcumin-zinc framework encapsulated microneedle patch for promoting hair growth. Theranostics, 13, 3675 - 3688.