
What is Acne?
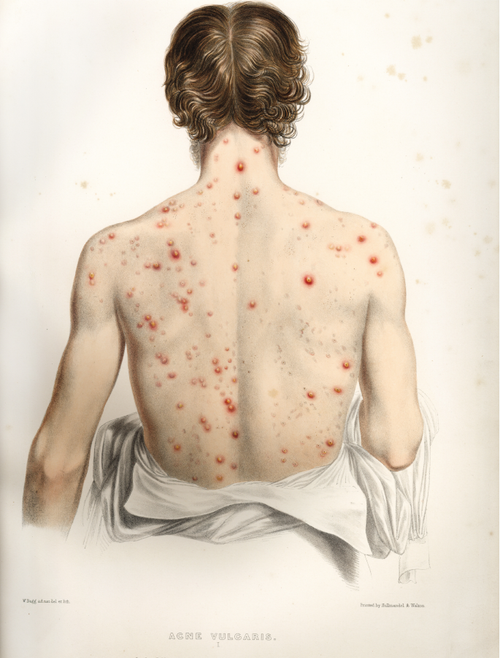
Acne, or acne vulgaris, is a common skin condition that happens when hair follicles (pores) get clogged with oil (sebum) and dead skin cells. This blockage can cause blackheads, whiteheads, pimples, and in more severe cases, painful nodules or cysts. Acne most commonly appears on the face but can also affect the chest, back, and shoulders.
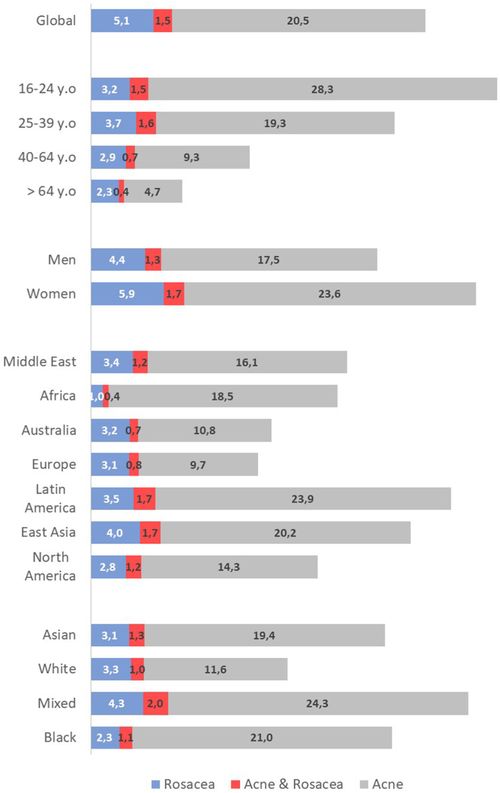
A recent global study of over 50,000 people aged 16 and older found that around 20.5% had acne, with the highest rates (28.3%) among those aged 16 to 24. Since the 1990s, the global burden of acne in adolescents and young adults has increased by 39.2%.
Types of Acne
Acne is generally classified into two main types: non-inflammatory and inflammatory.
Non-inflammatory Acne
- Whiteheads (closed comedones): Small white bumps caused by clogged pores that stay closed at the surface.
- Blackheads (open comedones): Small black or dark yellow bumps; the clogged pore is open, and its contents darken when exposed to air.
Inflammatory acne are red, swollen, and sometimes painful due to inflammation or infection.
- Papules: Small, red, tender bumps without pus.
- Pustules: Red bumps with a white or yellow center filled with pus.
- Nodules: Large, painful lumps deep under the skin caused by severe inflammation.
- Cysts: Deep, pus-filled, painful lumps that often lead to scarring, which is the most severe form of acne.

Other special types of acne include:
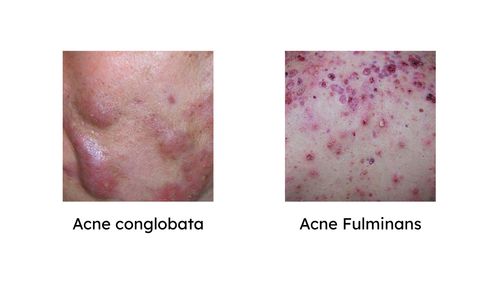
- Acne conglobata: A rare and severe form with large, interconnected lumps and cysts.
- Acne fulminans: A very rare and aggressive form that causes painful nodules and open wounds.
- Acne mechanica: Triggered by friction, pressure, or rubbing, leading to pimples in affected areas.
- Acne rosacea: Often mistaken for regular acne, it causes redness, visible blood vessels, and bumps on the nose and cheeks, but does not include blackheads or whiteheads.
The Word 'Acne'
The word 'acne' likely comes from a misspelling of the Greek word 'akme,' meaning 'peak' or 'point,' a reference to puberty. It was probably first used in the 6th century by Aetius Amidenus, a physician in Constantinople, who described facial lesions at the 'acme' of life. Due to the inconsistent spelling at that time, and the similarity between the letters 'm' and 'n' may have led to a transcription error—from akme to acne. Some also believe the word may have roots in other Greek terms for rashes or Egyptian words for boils and skin sores.
The term 'comedo' (used for blackheads and whiteheads) appeared in the 1600s–1700s, possibly linked to Latin or German words suggesting parasites or facial hair. It became more widely accepted in the 1800s.
Sebum comes from Latin, meaning 'fat' or 'tallow' and 'seborrhea' was introduced later by German doctor Conrad Heinrich Fuchs.
In the late 19th and early 20th centuries, acne was initially viewed primarily as a female concern, heavily influenced by cultural pressures linking clear skin to femininity. Young women, driven by anxiety over their appearance and motivated by vanity and emotional distress, often sought medical help, adhering diligently to treatments. During this period, acne was also associated with dirtiness and low social class, reflecting the growing emphasis on hygiene spurred by the germ theory of disease.
By the early 20th century, acne began to impact job prospects and military performance, with severe outbreaks in harsh wartime conditions causing physical pain and disability. This shift prompted the medical community to recognize acne as a significant health issue, particularly due to its effects on mental health and social functioning. Later, acne was recognized as a real health issue tied to adolescent mental health challenges, such as low self-confidence, emotional distress, and social exclusion. This recognition increased parental involvement, drew greater attention from the medical field, and opened new commercial opportunities.
Traditional vs. Modern Treatment
Traditional treatments date back as far as 1550 BC. One of the earliest mentions appears in the Ebers Papyrus from ancient Egypt, which recommended using raw honey and sulfur to treat acne. In ancient Greece, the physician Theodosius believed wiping the face with a towel while watching a falling star could help clear blemishes. The Romans also experimented with a wide range of remedies—including honey, sulfur, crocodile meat, cypress oil, sour cheese, leek leaves, cinnamon, and even bruised parsley, in hopes of finding a cure.
Other early treatments included skin peels and antiseptics, as noted in Cosmetic Dermatology. Some now-outdated methods even involved using crushed dry ice and laxatives, which are no longer considered safe or effective.
In 1877, American dermatologist Louis Adolphus Duhring categorized acne treatments into two types: general (addressing overall health) and local (focusing on the skin). He paid close attention to related issues like indigestion, constipation, and migraines. For stubborn skin bumps, he recommended applying carbolic acid. Mechanical treatments also emerged during this period, for example, rubbing the skin with sand to remove blackheads.
In late 19th-century Paris, doctors were experimenting with physically clearing pores using fine needles, then injecting iodine to dry the area, claiming spots could disappear within 24 hours.
In the early 20th century, acne was sometimes treated with ionizing radiation. However, this approach was abandoned due to cancer concerns. Around the same time, light therapy using quartz mercury vapor lamps gained popularity.
A major breakthrough came in the 1960s when the pharmaceutical company Roche tested a synthetic vitamin A compound, 13-cis-retinoic acid, originally for skin cancer. Although ineffective against cancer, it proved highly effective in treating acne. The U.S. FDA approved it for acne in 1982, followed by approval in Europe in 1983.
Meanwhile, Canadian dermatologist William Pace identified the acne-fighting potential of benzoyl peroxide, which has since become one of the most widely used topical treatments.
Mainstream vs. Alternative Views
Mainstream acne treatments focus on managing current breakouts by targeting key factors like excess sebum production, hyperkeratinization (clogged pores), and bacterial infection.
- Anti-inflammatory medications – such as Accutane (oral retinoids), azelaic acid, and nicotinamide.
- Antibacterial agents – including PanOxyl (benzoyl peroxide), antibiotics, and azelaic acid.
- Keratolytics (exfoliants) – like salicylic acid and Retin-A (topical retinoids), which help unclog pores.
- Hormonal therapies – used mainly in women to regulate oil production.
- Post-acne treatments – such as hydroquinone to reduce dark spots or scarring.
Some medications work in multiple ways. For example, azelaic acid, retinoids, and benzoyl peroxide offer both antibacterial and anti-inflammatory effects. Because of their versatility, these are among the most commonly prescribed treatments for acne.
Supportive treatments, such as light/laser therapy, cryotherapy (freezing treatments), comedone extraction, cryoslush therapy and intralesional corticosteroids may also be implemented in some cases.
What does science say?
Acne treatments target one or more of the main pathogenic factors: excess sebum production, abnormal skin cell turnover, bacterial colonization, and inflammation. Although these treatments can effectively manage acne, their side effects are noteworthy. Most of them commonly cause skin dryness, irritation, peeling, burning, or tingling. Some antibacterial agents may also lead to unpleasant gastrointestinal symptoms such as bloating, diarrhea, nausea, and vomiting. Hormonal therapies, in some cases, can worsen acne, alter skin type, cause pigmentation, or lead to excessive hair growth. Other reported side effects include mood changes, weight gain, blood clots, and hormone-related complications.
The effectiveness of certain acne medications can be influenced by dietary factors, which are often emphasized when prescribed.
Some acne medications, like isotretinoin (including Accutane) and spironolactone, are better absorbed when taken with high-fat meals (around 50 grams of fat). These drugs don’t dissolve well in the stomach alone but are much more effective when fat is present.
Newer versions of isotretinoin, like lidose-isotretinoin, are designed to dissolve better, even on an empty stomach and lower dose, due to improved formulation.
Calcium in milk can interfere with the absorption of antibiotics such as doxycycline, tetracycline, and minocycline. One study found that doxycycline absorption dropped by about 20% when taken with food. Milk and meals reduced absorption of minocycline and tetracycline, with tetracycline being the most affected. However, slow-release or delayed-release versions of these antibiotics are less impacted by food, and in some cases, may even absorb a bit faster.
Some early research has also suggested that whey protein (from dairy) might interfere with acne treatment results, but there’s no strong evidence to confirm this yet.
Minerals like calcium, magnesium, iron, zinc, and aluminum can all bind to tetracycline antibiotics in the stomach. This makes it harder for the body to absorb the medication, which can reduce how well it works. Among them, iron seems to especially affect minocycline.
Alternative
Dietary Patterns
Alternative perspectives on acne management often highlight the role of diet, natural substances, and holistic wellness in influencing acne progression. Several dietary patterns have been suggested to help improve acne, including low-carbohydrate diets.
- Low-carbohydrate diets
- Ketogenic diet
- Paleolithic (Paleo) diet
- Mediterranean diet
- Plant-based or vegan diets
What does science say?
Dietary patterns have long been considered in acne management, with growing interest in how certain eating habits may influence skin health. Among these, low-carbohydrate and low-glycemic index diets have consistently shown promising results, including a significant reduction in acne severity and lesion counts, especially in young individuals.
The ketogenic diet, which is high in fats and extremely low in carbohydrates, was originally developed for managing epilepsy, partly due to its effect on mTORC1 activity in the brain. Although evidence is still limited, a few studies have reported notable improvements in acne symptoms among individuals following ketogenic diets.
The Paleolithic (Paleo) diet, which emphasizes lean meats, fish, fresh fruits and vegetables, nuts, and seeds, has also been suggested as beneficial for acne. This idea was notably promoted by Loren Cordain in 2005. While the biochemical reasoning behind the Paleo diet’s potential effects on acne is well established, rigorous placebo-controlled clinical trials confirming its effectiveness are still lacking.
The Mediterranean diet, rich in whole grains, fruits, vegetables, olive oil, and fish, has shown potential in protecting against moderate-to-severe acne in some studies. Its anti-inflammatory and antioxidant properties are believed to underlie this effect.
The plant-based and vegan diets are gaining attention for their anti-inflammatory properties. Early findings suggest they may also contribute to clearer skin, although more robust evidence is still needed.
The rationale behind using dietary changes to improve acne centers on a shared concept: the quantity and composition of foods can influence sebaceous gland activity and hormonal function.
Diets high in glycemic load (GL) raise insulin demand, and over time, may lead to insulin resistance. Elevated insulin levels increase the production of IGF-1 in the liver, a hormone strongly linked to increased sebum production and acne development. Insulin may also indirectly stimulate androgen production, further worsening acne.
A very low-calorie ketogenic diet has been reported to improve insulin sensitivity, reduce inflammation, and offer antioxidant benefits. Even though it is slightly different from standard ketogenic diet but shares the goal of including ketosis. This matters because mTORC1, a protein complex involved in cell growth and inflammation, plays a central role in acne. It is activated by insulin, glucose, and certain amino acids such as leucine, which are abundant in meat and dairy.
By drastically lowering carbohydrate intake, ketogenic diets reduce insulin and glucose levels, which may in turn decrease mTORC1 activity and associated inflammation. While leucine remains in the diet, the hormonal and metabolic environment created by ketosis may help counterbalance its effects—potentially explaining the skin improvements seen in some keto followers.
Dietary fats, especially omega-3 fatty acids, have been shown to reduce IGF-1 levels and decrease sebum production and follicular blockage. Omega-3s are also known for their anti-inflammatory effects, which likely contribute to the benefits observed in Mediterranean diets. A randomized controlled trial using omega-3 and γ-linoleic acid supplements showed significant reductions in both inflammatory and non-inflammatory acne lesions compared to control groups. Conversely, high intake of trans fats and saturated fats has been associated with worse acne outcomes in some studies.
Dairy products, particularly those high in casein (a milk protein), have also been implicated in increased IGF-1 levels. Much of the data linking dairy to acne is based on self-reported intake, often involving ice cream and other processed foods, where dairy may not be the sole contributing factor. Some researchers suggest the glycemic impact of milk, rather than its fat or protein content, may be more relevant, once again linking back to insulin’s role in acne.
Nutrients
Beyond diet patterns, specific nutrients and supplements have gained attention for their potential benefits:
- Vitamins A to E
- Collagen supplements
- L-glutamine
- Zinc
- Probiotics
- Plant-derived polyphenols
What does science say?
Beyond overall dietary habits, certain vitamins and minerals have gained attention for their potential to help manage acne. Several studies have reported that individuals with acne tend to have lower levels of certain vitamins and minerals, including vitamins A, C, D, E and zinc, compared to those without acne. While some mechanisms are still under investigation, many proposed explanations are biologically plausible and supported by early evidence.
Vitamins C and E, along with plant-based compounds like polyphenols, are well known for their anti-inflammatory and antioxidant effects. Antioxidants help neutralize free radicals, unstable molecules that contribute to inflammation and skin damage. By reducing this oxidative stress, these nutrients may help calm inflamed skin and reduce acne breakouts. Several studies suggest that a diet rich in fresh fruits and vegetables—which are naturally high in antioxidants and vitamins, can lead to clearer, healthier skin.
Vitamin C, in particular, inhibits NF-κB (a key regulator of inflammation), supports wound healing, and reduces hyperpigmentation,making it useful for both active acne and post-acne marks. Although vitamin E alone shows limited benefits, its effects improve when combined with nutrients like gamma-linolenic acid, beta-carotene, coenzyme Q10, or grape seed extract. Plant-derived polyphenols may also modulate the gut microbiota, improve insulin sensitivity, and influence hormonal activity, all factors relevant to acne.
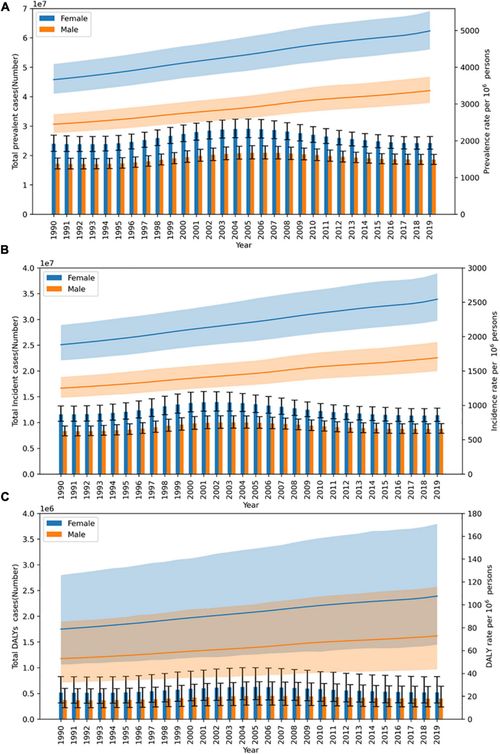
Trends of acne vulgaris in China from 1990 to 2019.
(A) Prevalent cases and rate. (B) Incident cases and rate. (C) Disability-adjusted life years (DALYs) cases and DALY rate.
Analysis of the epidemiological burden of acne vulgaris in China based on the data of global burden of disease 2019.
Vitamin A plays a vital role in maintaining the skin’s natural barrier and regulating cell turnover. Its synthetic derivatives, known as retinoids (commonly known in brand name Accutane), are widely used in acne treatment. One of the most effective forms, isotretinoin (a specific oral retinoid), works by reducing sebum production and preventing excessive skin cell buildup, which helps limit the growth of Cutibacterium acnes. Studies have shown that increased vitamin A levels are linked to significant improvements in both inflamed and non-inflamed acne lesions.
Low vitamin D levels have been linked to acne, though definitions of deficiency and confounding factors have led to mixed findings. However, several randomized trials show that vitamin D supplementation in deficient individuals can significantly reduce inflammatory lesions and cytokine levels. Vitamin D’s benefits are tied to its anti-inflammatory and immune-regulating properties, which help reduce sebum production, prevent clogged pores, and inhibit C. acnes growth.
Zinc has gained attention in acne management due to its low cost, minimal side effects, and potential effectiveness. Several studies have reported that oral zinc sulfate treatment can lead to a modest reduction in the number and severity of acne lesions compared to placebo. However, results are mixed, other studies have shown little to no clinical benefit, highlighting the need for more consistent evidence before zinc can be considered a reliable standalone treatment.
The potential benefits of zinc are thought to come from its anti-inflammatory and antibacterial properties. While the exact mechanisms remain unclear, zinc may help regulate immune function, inhibit the growth of Cutibacterium acnes, and support wound healing in acne-prone skin. These combined actions might explain the improvements seen in some studies.
B vitamins, particularly B12 and B6, have a complex relationship with acne. High doses of B12 can trigger or worsen breakouts in some individuals, as supplementation alters C. acnes gene expression, leading to increased
porphyrin production, a cause of skin inflammation. Similarly, high doses of B6 have been linked to acne-like eruptions, though this is less frequent than with B12.
At appropriate doses (50–250 mg/day), vitamin B6 can reduce sebum production and regulate sex hormones, which may benefit hormonal acne.
Vitamin B6 (pantothenic acid) also shows promise: oral supplementation has reduced both inflammatory and non-inflammatory acne in mild to moderate cases. B5 supports lipid metabolism and skin barrier integrity via coenzyme A (CoA), and it exerts anti-inflammatory effects.
While bacteria on the skin, like Cutibacterium acnes, have long been linked to acne, researchers are now paying more attention to what's happening inside the body, especially in the gut. This idea is known as the gut-skin axis, and it suggests that the balance of bacteria in the digestive system may affect inflammation and immune responses throughout the body, including skin. People with acne have been found to have higher endotoxin levels, molecules that trigger inflammation, compared to those without acne.
Probiotics and fermented foods (yogurt, kefir, kimchi, miso, sourdough) may help improve gut health. Though most of the research so far has been done on animals or outside of the body, the results are promising. For example, giving certain probiotics (like Bifidobacterium lactis) to diabetic mice helped improve blood sugar control and insulin levels. Other studies found that combining probiotics, such as Lactobacillus casei, Lactobacillus bulgaricus, and Streptococcus thermophilus, with healthy fats increased levels of anti-inflammatory compounds in the body. Gut bacteria also seem to influence key biological pathways, like
mTOR signaling, which is linked to both metabolism and acne development. In one small human study, 20 adults with acne took a probiotic drink containing
Lactobacillus rhamnosus GG daily for 12 weeks. Compared to those who took a placebo (a similar drink without probiotics), the probiotic group saw noticeable improvements in their skin. Skin samples also showed lower levels of IGF-1 and higher expression of a gene called
FoxO1, which helps regulate skin health. While these early results are encouraging, more research is needed to fully understand the benefits.
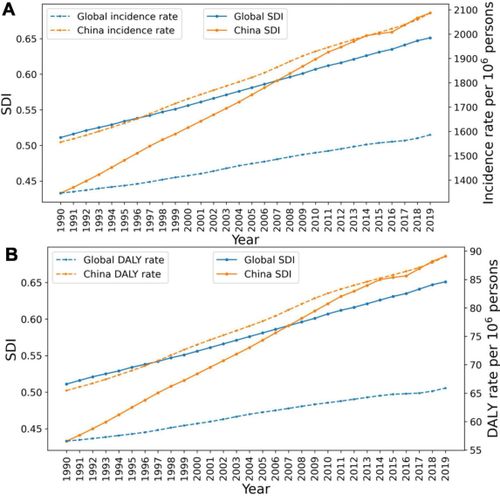
The relationship between acne vulgaris and sociodemographic index (SDI) in China and around the world.
(A) The relationship between age-standardized incidence rate of acne and SDI. (B) The correlation between acne disability-adjusted life year (DALY) rate and SDI.
Analysis of the epidemiological burden of acne vulgaris in China based on the data of global burden of disease 2019.
Collagen and L-glutamine have gained attention in acne management, mostly for their roles in supporting overall skin health and reducing inflammation. Collagen, the primary protein responsible for skin firmness and repair, is particularly noted for its potential in post-acne recovery. While current evidence does not strongly support collagen supplements for preventing or treating active acne, both topical and injectable collagen therapies have demonstrated clear benefits in improving atrophic (indented) acne scars by stimulating tissue repair and filling depressed areas.
L-glutamine, on the other hand, supports gut barrier function and immune balance, which could indirectly benefit acne through the gut-skin axis. Its potential to reduce systemic inflammation has led to its frequent mention alongside probiotics in acne-related discussions.
For L-glutamine, one small clinical study found that a supplement containing L-leucine, L-arginine, and L-glutamine improved skin texture and barrier function in healthy young women, possibly due to L-glutamine’s role in gut health and its conversion to
glutathione, an antioxidant. However, this study did not involve individuals with acne, and there is currently a lack of high-quality clinical trials directly evaluating L-glutamine’s effectiveness in acne treatment. Interestingly, some metabolic profiling research has even suggested L-glutamine may play a role in acne development, emphasizing the need for further investigation.
Traditional remedies
Additionally, several natural and traditional remedies have been explored:
- Royal jelly
- Chinese herbal medicine (e.g., Dang Gui)
- Evening primrose oil
What does science say?
Some natural remedies, such as royal jelly and evening primrose oil, have been suggested as supportive treatments for acne due to their anti-inflammatory and antibacterial properties.
Royal jelly, a creamy, nutrient-rich secretion produced by worker honeybees to feed queen bees and young larvae, has shown to stimulate collagen production and support skin cell renewal, which may help repair damaged skin and reduce the appearance of acne scars. Several reviews and clinical trials have highlighted its strong antibacterial and anti-inflammatory effects, both of which are valuable in reducing acne-causing bacteria and calming inflamed breakouts. Notably, royal jelly has also been found to prevent the release of pro-inflammatory cytokines in mouse macrophage cultures without harming the cells.

Evening primrose oil contains gamma-linolenic acid (GLA), an omega-6 fatty acid that may help reduce inflammation and improve symptoms of hormonal acne. While it shows some benefit in supporting skin hydration and healing, its effects tend to be more consistent when used alongside conventional treatments, such as isotretinoin, rather than as a stand-alone remedy.
Traditional Chinese herbal medicine (TCM) has also shown promise in supporting acne treatment. Dang Gui (Angelica sinensis), for instance, is well known in TCM for its blood-tonifying and moistening properties. In TCM theory, these actions are believed to promote healing of slow-healing sores, reduce inflammation, and improve skin conditions related to blood deficiency and stagnation, factors that may support acne recovery and lessen lesion severity.

Dragon Herbs
A clinical study evaluated treatments for acne vulgaris and included a group treated with Dang Gui Ku Shen Wan, a formula containing Dang Gui and Sophora root. Although this treatment was less effective than the experimental compound used in the study, it still demonstrated a notable therapeutic benefit, with a combined cure and significant improvement rate of 47.06%. Further analysis of Dang Gui has identified multiple active compounds in Dang Gui that may influence acne-related biological pathways, such as inflammation, sebaceous glands regulation, and oxidative stress, all of which are important in acne development and treatment.
Who gets Acne?
Considering age
Acne isn't just a teenage problem—it can affect people of all ages. While many start experiencing acne during adolescence, a significant number of adults continue to deal with it later in life, or even develop it for the first time as adults. On the other end of the spectrum, acne can also appear in very young children, including newborns, infants, and preteens, though it's less common in those groups.
Considering gender
Women tend to experience acne more often than men, and this holds true across all age groups. Hormonal changes related to menstruation, pregnancy, and other life stages may contribute to this difference.
Considering ethnicity
Research shows acne affects people of all skin types. One study reported acne in about 27.7% of Black individuals and 29.5% of Caucasians. In the UK and Singapore, adult acne was found in 13.7% of Black patients and 10.9% of Indian and Asian patients. Globally, acne tends to be more common in East Asia, Latin America, and the Middle East, and less common in Europe and Australia. Rates in North America and Africa were about the same.
Interestingly, some traditional or isolated groups, like the Canadian Inuit, South African Zulus, Japanese Okinawans, the Aché of Paraguay, and Kitavan islanders of Papua New Guinea, were historically reported to have little to no acne, which has sparked scientific curiosity.
Considering lifestyle
The connection between lifestyle choices, like smoking, and acne isn't fully clear, with studies showing mixed results. In contrast, diet has been a topic of debate for decades. Some researchers believe that nutrition may affect acne by influencing hormone levels, especially
IGF-1. Diets that are low in sugar, rich in omega-3 fatty acids, or that limit dairy intake have been suggested to help.
However, others argue that the evidence is weak or outdated. One major challenge is that it's hard to control diets in studies, especially with teenagers. As a result, although there are promising findings, there's still no scientific consensus due to the lack of large, high-quality studies.
The Kitavan Islanders of Papua New Guinea and the Aché hunter-gatherers of Paraguay were once believed to have low rates of acne due to their genetics. But researchers later discovered that people with similar ethnic backgrounds, like other South American Indigenous groups and Pacific Islanders, who had adopted Western lifestyles actually had much higher rates of acne.
This suggests that genetics alone don’t explain the difference. Instead, diet and lifestyle likely play a major role. The Kitavan and Aché people typically eat more omega-3-rich foods, low-glycemic meals, and very little dairy, all of which have been linked to a lower risk of acne.
Considering genetics and hormones
Genetics and hormones also influence acne. People with certain conditions, like
polycystic ovary syndrome (PCOS), high testosterone levels, or elevated cortisol, are more likely to have acne. Research also shows that acne tends to
run in families and can be more severe in
identical twins, which suggests a strong
genetic link.
Considering environment
Environmental conditions can significantly influence acne severity. High temperatures have been shown to increase sebum production, which can lead to more frequent or severe breakouts. In addition,
exposure to ultraviolet (UV) rays
can
thicken the outer layer of the skin, potentially
clogging pores
and worsening acne through blockage of the pilosebaceous units.
Compared to preindustrial times,
global average temperatures have risen by approximately 1.1°C
largely due to
climate change driven by human activities.
This warming trend may contribute to environmental conditions that aggravate acne for some individuals.
Notes for Conventional Treatments
Most conventional standard acne treatments require a doctor’s prescription, and it is best to use medications under professional supervision due to individual health considerations.
Pregnant women should follow a stepwise treatment approach tailored to acne severity and gestational age, given the potential risks to the fetus. Oral retinoids and hormonal agents are strictly contraindicated because of their high teratogenicity (the ability of a drug to cause fetal abnormalities or deformities). Salicylic acid should also be used with caution, particularly in high concentrations, due to the risk of systemic absorption.
Women of childbearing age who are not currently pregnant should also exercise caution, as oral retinoids carry a significant risk of birth defects if conception occurs during treatment.
Certain antibiotics, such as doxycycline and minocycline, should be avoided in
children and adolescents
due to the risk of bone growth inhibition and tooth discoloration.
Synergistic Pairings
Fats
It is generally recommended to take Accutane (isotretinoin) or spironolactone with a high-fat meal to enhance absorption.
Dairy
Avoid consuming dairy products when taking acne antibiotics such as doxycycline, tetracycline, or minocycline, as they can reduce the medication’s effectiveness.
Minerals
For optimal absorption, avoid taking mineral supplements or antacids for
2–3 hours
before
and
2 hours after
using these antibiotics.
Common Questions
Should I pop pimples or leave them alone?
It is generally best to leave pimples alone and avoid popping them. Squeezing or picking at them can make things worse by causing infection, scarring, or slower healing. Instead, focus on gentle care and proven treatments. If breakouts are severe or don’t improve, consider seeing a dermatologist.
- Hands off: Avoid touching, squeezing, or picking at pimples—it can push bacteria deeper and leave marks.
- Gentle cleansing: Wash your face twice a day with a mild, non-irritating cleanser.
- Warm compress: For painful pimples, apply a warm (not hot) compress to reduce discomfort and help them heal naturally.
Does the birth control pill interact with acne? Is it worth it to reduce acne with the pill, given the side effects of the pill?
The combined birth control pill
(containing both estrogen and progestin) has been scientifically shown to reduce acne. It works by regulating hormones, especially by lowering the activity of androgens, which are hormones that can increase sebum production and lead to breakouts. As a result, many people notice less oily skin and fewer pimples while on the pill.
Only combined pills (estrogen + progestin) are helpful for acne. Progestin-only options, like the “mini-pill” or certain implants, can sometimes make acne worse.
Possible side effects of birth control pills include: Breast tenderness
- Nausea
- Headaches
- Mood changes
- Irregular bleeding
- Changes in weight or sex drive
There are also rare but serious risks, such as an increased chance of blood clots, especially for women over 35 who smoke. The severity and likelihood of side effects can vary from person to person. And it often takes
3–6 months
to see noticeable improvements in acne when using the pill.
So, it's best to talk with a healthcare professional about your medical and family history, as well as the risks and benefits, if this is something you are considering.
What are the side effects of Accutane? Can I reduce the severity of side effects of Accutane?
Accutane (isotretinoin) can be highly effective for severe acne, but it often comes with side effects. The most common ones include: Dry skin (may feel tight, red, or flaky)
- Dryness of the lips, eyes, and inside the nose
- Changes in hair or nails (such as thinning or brittleness)
- Joint or muscle pain
Some might worry that liver toxicity due to long-term consumption, however, Accutane can cause temporary elevation in liver enzymes and might show abnormal results in liver blood tests; these changes are usually mild, reversible, and rarely result in lasting liver damage.
To reduce the side effects:
- Work with your dermatologist on the right dose – lower doses are usually linked to fewer side effects.
- Keep your skin hydrated – use fragrance-free, non-comedogenic moisturizers regularly.
- Use a gentle cleanser – avoid harsh scrubs or products that can irritate your skin.
- Protect your skin from the sun – apply a broad-spectrum sunscreen daily, wear protective clothing, and limit direct sun exposure, as Accutane can make your skin more sensitive to sunlight and UV rays.