
What is Vitamin A (Retinol)?
Vitamin A is a generic term for retinol and its related compounds in different active forms. Dietary vitamin A can be consumed either as preformed vitamin A (retinol) or provitamin A, including beta-carotene and certain other carotenoids. Preformed vitamin A is usually found in animal sources, while provitamin A is mainly found in bright-colored plant-based sources. Vitamin A is essential for visual function, cellular differentiation, growth, reproduction, bone development and immune system health. Since mammals cannot produce vitamin A on their own, we must rely on dietary sources to maintain adequate levels. Additional sources include supplements and medications. For example, Accutane, a prescription treatment for acne, contains retinoids, which are derivatives of vitamin A. Meanwhile, synthetic forms, retinyl esters including retinyl palmitate, retinyl acetate and synthetic beta-carotene are commonly used in fortified foods and supplements.
Example dietary sources
Table 1: Vitamin A and beta-carotene contents of selected foods.
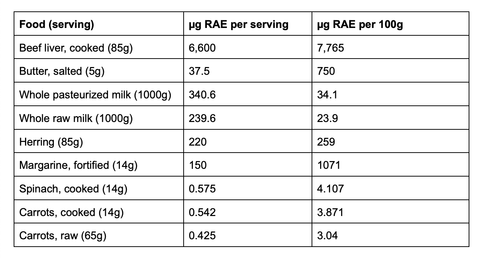
Standard conversion of vitamin A: 1 μg RAE = 1 μg retinol, 2 μg beta-carotene from supplements, 12 μg beta-carotene from foods.
- 1 International Units (IU) vitamin A = 0.3 μg RAE.
- 1 IU supplemental beta-carotene = 0.3 μg RAE.
- 1 IU dietary beta-carotene = 0.05 μg RAE.
Retinol vs. beta-carotene, what's the difference?
Besides the sources and types, the biggest difference between retinol and beta-carotene is how the body absorbs them. Retinol can be directly taken up in the intestine, whereas beta-carotene needs to be converted into retinol first, which makes it less efficient. Therefore, they also differ in effectiveness and bioavailability.
A brief history
English biochemist Frederick Gowland Hopkins made pioneering observations on vitamins. He found that rats struggled to survive on a diet consisting only of pure protein, carbohydrates, fats, and salts but were able to grow normally when milk was included. This led him to propose the existence of “unsuspected dietetic factors” essential for normal growth, laying the foundation for the discovery of vitamins.
Key events and scientific milestones
The modern era of vitamin A research began in 1913 with the independent discoveries of 'fat-soluble A' by American biochemists Elmer Verner McCollum, Marguerite Davis, and Lafayette Mendel. They found that rats could not grow normally on a diet consisting only of isolated protein, starch, lard, and “protein-free” milk but were able to grow into young rats when butter was used instead of lard. In 1931, Swiss chemist Paul Karrer described the chemical structure of vitamin A. Retinoic acid and retinol were first synthesized in 1946 and 1947 by two Dutch chemists, David Adriaan van Dorp and Jozef Ferdinand Arens.
Picture: George Wald
Credit: IMD
The chemical processes of vision in the eye were discovered by American scientist George Wald in 1967. His research explained how our eyes use a light-sensitive molecule to detect light and send signals to the brain, allowing us to see in the dark. Further research by German physiologists Wilhelm Kühne and Franz Christian Boll led to the discovery and confirmation of a light-sensitive pigment called visual purple, refining the understanding of how human vision works in low-light conditions.
Traditional vs. modern usage
More than 2,000 years ago, Egyptian physicians treated night blindness by squeezing the juice of a grilled lamb’s liver into patients’ eyes, unaware of vitamin A or its role in vision. The choice of animal liver may have been influenced by availability. In 17th-century China, pig liver was commonly used, while around 300 BC in Greece, it was recommended to consume “raw beef liver, soaked in honey, to be taken once or twice daily by mouth” as a delicacy. As early as 2500 BC, the ancient Egyptians discovered that birds could be fattened by overfeeding and started this practice, although it's unclear if they specifically sought the fattened livers as a delicacy. Over time, this practice spread across Europe. By the 17th and 18th centuries, foie gras had become a key part of French cuisine, made from the livers of ducks or geese and sold whole or turned into mousse, parfait, and pâté. Today, foie gras is officially recognized by law as part of France’s protected cultural and culinary heritage.

Picture: Liver Pâté
Credit: ChatGPT
Today, vitamin A fortification is a common strategy for managing vitamin A deficiency. Margarine is the most commonly fortified product, with fortification being mandatory in the United Kingdom and the United States. Some European Union countries, like the Netherlands, Finland, Belgium, Poland, and Sweden, encourage adding vitamin A to margarine, without the EU-wide rule to make it a requirement. Moreover, breakfast cereals, milk, and dairy products are usually voluntarily fortified. To ensure even distribution in low-fat or skim milk, vitamin A is typically dissolved in seed oils before being incorporated. In places where vitamin A deficiency is a bigger problem, like Southeast Asia and Africa, more everyday foods are fortified to help people get enough. These include rice, soy sauce, instant noodles, sugar, and MSG.
Mainstream vs. Alternative Views
Vitamin A deficiency is a major public health problem, commonly found in developing countries, but rarely seen in developed countries. It is typically caused by unbalanced diets with limited food variety and inadequate access to vitamin A-rich foods. One of its primary symptoms is night blindness, which can lead to total blindness in severe cases. Other symptoms include xerophthalmia (dry eye condition), weight loss, keratinized skin (rough, dry, or thickened skin) and so on. It can also increase risk of anemia and weaken the immune system. Since vitamin A is essential for cell development, vision, growth, and normal metabolism, its deficiency can significantly impair tissue function especially during critical periods, such as infancy, childhood, pregnancy and lactation. The WHO is still developing specific recommendations for vitamin A fortification of staple foods.
Concerns exist about vitamin A toxicity due to its fat-soluble nature, which can lead to accumulation in the body. This increases the risks from long-term supplementation, frequent consumption of fortified foods, and/or high liver intake. Additionally, chronic vitamin A toxicity is often underdiagnosed because its symptoms are frequently mistaken for other conditions, which include fatigue, dry skin, joint pain and headaches. Alternative health writer Grant Genereux suggested that vitamin A toxicity is responsible for a range of chronic diseases and has advocated for a low-vitamin A diet.
Consuming excessive amounts of retinol can lead to hypervitaminosis A, which is classified into acute and chronic forms. Acute toxicity typically results from a large, sudden intake of synthetic forms of vitamin A, such as supplements and medications, while chronic hypervitaminosis A occurs from long-term consumption of lower, but still excessive amounts of vitamin A, from supplements, foods, or self-medication with vitamin A preparations.
Synthetic (lab-produced) vitamins are usually similar or identical in chemical structure to natural vitamins but often have lower bioavailability. This is because natural sources contain other nutrients that may enhance absorption through synergistic interactions. One common form of synthetic vitamin A is retinyl esters, which is also the storage form in the liver. The absorption of preformed retinyl esters from dietary supplements is 70%–90%, and that of beta-carotene ranges from 8.7%–65%.
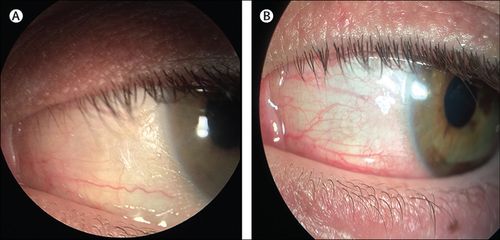
Picture: Eye change caused by vitamin A deficiency
(A) Dry, grey, thickened outer eye surface (called conjunctiva), showing signs of dryness. (B) The dryness improved after treatment with vitamin A and other supplements.
Credit: Vitamin A deficiency—an unexpected cause of visual loss
Reported cases of vitamin A toxicity are rare, averaging fewer than 10 per year from 1976 to 1987. The lack of updated data may be due to the condition being difficult to diagnose and often overlooked as a cause. Most research focuses on short-term, acute effects in animals, often using injections, which may not accurately represent how the body processes vitamin A from food and supplements. The conversion of carotenoids to vitamin A in the body depends not just on a person's vitamin A levels, but also on the types and amounts of carotenoids consumed. Additionally, genetic differences, gut microbiome diversity, and the foods eaten alongside vitamin A are suggested to influence the effectiveness of conversion.
General populations
A varied and balanced diet typically provides sufficient vitamin A for most people. In some cases, fortified foods and dietary supplements can be helpful when it's difficult to meet nutrient needs through food alone.
Pregnant or planned to become pregnant
National dietary guidelines tend to suggest avoiding liver, liver products, and supplements or medications containing vitamin A, such as fish oil, unless recommended by your healthcare provider. Excessive vitamin A intake (from all sources) can lead to birth defects, including malformations of the eyes, skull, lungs, and heart. However, pregnant women in low-income and middle-income countries, or those with vitamin A deficiency, may require additional vitamin A to support both their own health and their baby's growth.
Lactation
Lactating women in low-income and middle-income countries, or those with vitamin A deficiency, may require additional vitamin A to ensure the sufficient vitamin A content in breast milk to meet infants’ needs for the first 6 months of life.
Menopause women and older men
Menopause women and older men, who are more at risk of weak bones, should avoid having more than 1500 μg of vitamin A a day from food and supplements, as suggested by the NHS. Research from animal, human, and laboratory studies generally supports the link between high vitamin A intake and bone mineral density loss, which is considered a risk factor for osteoporosis. However, some studies suggest that the source of vitamin A may play a role, while others do not.
Individuals with digestive issues
Individuals with cystic fibrosis, Crohn’s disease, and ulcerative colitis are at a higher risk of vitamin A deficiency. However, the effectiveness of vitamin A supplementation in improving vitamin A levels in these groups has shown inconsistent results.
Medications
Vitamin A can interact with certain medications, potentially affecting their absorption, effectiveness, or increasing the risk of side effects. These include: Orlistat (weight-loss medication); Anticoagulants (drug that prevent blood clots); Bexarotene (Targretin) (topical cancer drug); Hepatotoxic drugs (drugs that can harm liver, such as Paracetamol and Statins).
How to stack it?
Daily recommendation
There is no single global standard for vitamin A intake. General guidelines typically recommend: Adult men: 700–900 μg RAE/day; Adult women: 600–700 μg RAE/day. For women who are pregnant, or who intend to become pregnant, suggestions vary across regions, with 770 μg RAE/day suggested by National Institutes of Health, 700 μg RAE/day suggested by the European Food Safety Authority. For personalized recommendations, it's best to consult your national health authority, as requirements may vary based on local diets and health policies.
Upper limit
The National Academy of Medicine (USA) recommends an upper limit of 3,000 μg RAE/day for adults, including retinol from food, supplements, and beta-carotene.
Synergistic pairings
Fats: It has been found that both retinol and beta-carotene are better absorbed when the meal contains about 10 grams (or more) of fat.
Vitamin E
High beta-carotene intake may lower plasma vitamin E concentrations, as they compete for similar absorption and metabolism pathways in the body.
Vitamin K
Excess vitamin A consumption interferes with vitamin K absorption.
Iron
Iron plays a key role in converting beta-carotene into retinol (the oxidized form of retinol), the active form of vitamin A. Inadequate iron levels can make this conversion less efficient, potentially affecting vitamin A status in the body.
Zinc
Vitamin A transport in the body depends on two key vitamin A-binding proteins, which require zinc for protein synthesis. A lack of zinc can impair vitamin A transport. Zinc is also essential for an enzyme involved in converting beta-carotene into retinol.
Protein
Protein is necessary for the conversion of beta-carotene into vitamin A. Inadequate protein intake can reduce the efficiency of this process.
If your goal is to increase vitamin A (retinol) intake, rich sources like liver and dairy are ideal. For those following a plant-based diet, options include brightly colored vegetables such as spinach and squash. There is no clear consensus on the benefits of supplementing with synthetic retinol, as absorption and effectiveness can vary. A well-balanced diet with diverse sources of vitamin A is generally the best approach to maintaining optimal levels.
This article is for informational purposes only and does not constitute medical advice. Consult a healthcare provider before making changes to your health routine.